
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Judge’s order requiring hospital to give COVID patient ivermectin called “unethical”
- Thread starter JournalBot
- Start date
blackhawk887
Ars Legatus Legionis
Independent studies show promise for Ivermectin, if we look at actual data (a summarized site pooling all studies
If you summarize low quality studies you get low quality results.
If you summarize a mix of high and low quality studies, you also get low quality results.
The only way to get high quality meta-analyses is to restrict the review to high quality studies. We don't at the moment, have either of those.
And "shows promise" is a very low bar and not nearly enough to qualify as standard of care.
Upvote
16
(17
/
-1)
People, even scientists, go absolutely nuts when talking about drugs. How is it ok to consume dangerous drugs like alcohol and tobacco, but forbidden to take ivermectin? There are absolutely no studies that prove ivermectin does or does not work. Why is it your decision, that of the fda or anyone else to dictate whether this drug can be given? Sorry folks, but the fda has gotten it wrong many many times. Need I cite the opioid epidemic and the massive over-prescribing of narcotics in very recent times? It should be my decision, and mine alone, to decide what drugs I take in extremis. Although I concede ivermection is unproven, does that mean I should be forbidden to take it if there is any chance whatsoever that it might help?
This is the same bullshit argument propounded by anti-vaxxers, but in reverse.
Here, it's "there's an (unproven) chance it might work" ignoring the proven virtual certainty it'll make things worse.
With anti-vaxxers, it's "but the vaccine might cause me damage" ignoring the minuscule probability of that possibility versus the exponentially larger chance of the disease causing inordinately more damage.
Upvote
21
(21
/
0)
Post content hidden for low score.
Show…
I thought about this... If I and my wife were in the situation. She would want to help me, any way she can. I wouldn't want Ivermectin, and I wouldn't want her to pay any money to scammers. On the other hand, I would want her to know that she's done to help me.
So if she asks the hospital to treat me with Ivermectin, the best outcome would be that they tell her they are doing it, but not give me anything. It makes her happier, it doesn't hurt me, and it doesn't cost any money.
That would be completely unethical, and if it came to light risks the doctors getting their license revoked & the hospital getting sued. You do not get to lie to the patient and/or their decision maker about the treatment being given. Flat out.
Upvote
17
(17
/
0)
People, even scientists, go absolutely nuts when talking about drugs. How is it ok to consume dangerous drugs like alcohol and tobacco, but forbidden to take ivermectin? There are absolutely no studies that prove ivermectin does or does not work. Why is it your decision, that of the fda or anyone else to dictate whether this drug can be given? Sorry folks, but the fda has gotten it wrong many many times. Need I cite the opioid epidemic and the massive over-prescribing of narcotics in very recent times? It should be my decision, and mine alone, to decide what drugs I take in extremis. Although I concede ivermection is unproven, does that mean I should be forbidden to take it if there is any chance whatsoever that it might help?
There is no evidence ivermectin can help. Doctors aren't going to give you every random medicine you request just because you're desperate.
More to the point, this doctor is prescribing insane amounts of ivermectin, well beyond the accepted safe dosage.
Upvote
28
(29
/
-1)
For the next "alternative to medicine" cure, we need to push something that causes sterility in humans.
Upvote
10
(10
/
0)
People, even scientists, go absolutely nuts when talking about drugs. How is it ok to consume dangerous drugs like alcohol and tobacco, but forbidden to take ivermectin? There are absolutely no studies that prove ivermectin does or does not work. Why is it your decision, that of the fda or anyone else to dictate whether this drug can be given? Sorry folks, but the fda has gotten it wrong many many times. Need I cite the opioid epidemic and the massive over-prescribing of narcotics in very recent times? It should be my decision, and mine alone, to decide what drugs I take in extremis. Although I concede ivermection is unproven, does that mean I should be forbidden to take it if there is any chance whatsoever that it might help?
Thank you for your opinion Dr. Mengele. For the sane part of humanity, we'd like some evidence that the treatment is safe and effective rather than trying random human experimentation.
There's LOADS of things that "might" help covid. Cyanide. Massive doses of radiation. Methyl mercury. Is this really a path you want to go down?
Upvote
28
(28
/
0)
blackhawk887
Ars Legatus Legionis
People, even scientists, go absolutely nuts when talking about drugs. How is it ok to consume dangerous drugs like alcohol and tobacco, but forbidden to take ivermectin? There are absolutely no studies that prove ivermectin does or does not work. Why is it your decision, that of the fda or anyone else to dictate whether this drug can be given? Sorry folks, but the fda has gotten it wrong many many times. Need I cite the opioid epidemic and the massive over-prescribing of narcotics in very recent times? It should be my decision, and mine alone, to decide what drugs I take in extremis. Although I concede ivermection is unproven, does that mean I should be forbidden to take it if there is any chance whatsoever that it might help?
Hospitals and doctors have legal and ethical obligations to not harm patients. They are in no way obligated to give the patient any drugs they want.
Ivermectin is about 1,000 times as toxic as alcohol.
Upvote
26
(26
/
0)
Post content hidden for low score.
Show…
Statistical
Ars Legatus Legionis
Independent studies show promise for Ivermectin, if we look at actual data (a summarized site pooling all studies
If you summarize low quality studies you get low quality results.
If you summarize a mix of high and low quality studies, you also get low quality results.
The only way to get high quality meta-analyses is to restrict the review to high quality studies. We don't at the moment, have either of those.
And "shows promise" is a very low bar and not nearly enough to qualify as standard of care.
Not at all advocating for this being first course (or even advocating this at all for treatment) but not sure how we get past the politics of this and actually get what would be considered by, let's say you, high quality analysis.
I have no dog in the fight but I can say with 100% accuracy (anecdotally) which side of the political spectrum someone falls on based on this drug alone which doesn't make for good science. I don't think monthly booster shots get's us out of this pandemic so I welcome different ideas.
There is a clinical trial to use this drug in small doses AT THE ONSET of covid infection. It is likely based on prior studies the impact will be small. That even assumes the trial is successful the vast majority of trials fail. Even if successful it may have the most use in countries where vaccines aren't available in sufficient quantity to bridge the gap. Vaccines not only reduce the chance of infection they also quite massively reduce the chance of severe symptoms, hospitalization, and death. Essentially everything you could hope this drug does vaccines do it better. Much much better.
This drug isn't going to move the needle on the pandemic globally in the long run. The only way to get ahead of this pandemic is through vaccination. So either people stop clinging to their freedumb and dreams of guzzling toxic doses of horse dewormer as a last ditch hail mary once they get the "hoax" disease they could have been vaccinated against or this rages on for years and years. Millions of people dying for absolutely nothing. A completely preventable disease.
In the case of this patient the drug isn't even indicated for a clinical trial. Doses low enough to be safe would be utterly insufficient against a disease rapidly reproducing unchecked. This patient very likely could have been saved by a vaccine BEFORE getting infected not loading up with toxic doses of horse dewormer in the terminal stage.
Upvote
19
(19
/
0)
People, even scientists, go absolutely nuts when talking about drugs. How is it ok to consume dangerous drugs like alcohol and tobacco, but forbidden to take ivermectin? There are absolutely no studies that prove ivermectin does or does not work. Why is it your decision, that of the fda or anyone else to dictate whether this drug can be given? Sorry folks, but the fda has gotten it wrong many many times. Need I cite the opioid epidemic and the massive over-prescribing of narcotics in very recent times? It should be my decision, and mine alone, to decide what drugs I take in extremis. Although I concede ivermection is unproven, does that mean I should be forbidden to take it if there is any chance whatsoever that it might help?
Hospitals and doctors have legal and ethical obligations to not harm patients. They are in no way obligated to give the patient any drugs they want.
Ivermectin is about 1,000 times as toxic as alcohol.
Next time I'm in the hospital, I wonder if they'll give me meth on demand?
Upvote
23
(23
/
0)
Post content hidden for low score.
Show…
Uh, "simple"? As a dual boarded physicia, trust me a multi-day written test is hardly simple... And all the people clamoring for his license getting revoked, don't seem to understand licensing and credentialing. That article doesn't mention if that doctor even has privileges at this ICU. I mean as a hospitalist my job is taking care of patients in the hospital for their outpatient providers. The outpatient providers (in general) have no ability to actually write an order that can be executed here in the hospital (I mean they can write a prescription all they want but that's an outpatient thing, I write orders - key difference is prescriptions are administered by the patient to themselves whereas orders are administered by the nurses to the patient). You need hospital privileges to do the latter but just a medical license and DEA # to do the former. But as an inpatient physician I am under no obligation to honor an outpatient prescription.Kind of irrelevant. The question is, as usual, why cannot we take away medical licenses when there is clear cause?That's ummm, disturbing.
And why is Dr. Wagshul still board certified?
Initial board certification is a simple test (also requires relevant residency experience). Mostly useful hanging on a wall, or seeking hospital privileges. Doesn't stop you from practicing medicine.
Upvote
22
(22
/
0)
blackhawk887
Ars Legatus Legionis
Independent studies show promise for Ivermectin, if we look at actual data (a summarized site pooling all studies
If you summarize low quality studies you get low quality results.
If you summarize a mix of high and low quality studies, you also get low quality results.
The only way to get high quality meta-analyses is to restrict the review to high quality studies. We don't at the moment, have either of those.
And "shows promise" is a very low bar and not nearly enough to qualify as standard of care.
Not at all advocating for this being first course (or even advocating this at all for treatment) but not sure how we get past the politics of this and actually get what would be considered by, let's say you, high quality analysis.
I have no dog in the fight but I can say with 100% accuracy (anecdotally) which side of the political spectrum someone falls on based on this drug alone which doesn't make for good science. I don't think monthly booster shots get's us out of this pandemic so I welcome different ideas.
There is no politics in what constitutes a high quality medical study. It needs to be a clinical trial, it needs to be randomized and placebo controlled, it needs to examine relevant dosages, it needs to be double-blinded, and it needs a large sample size - at least thousands, preferably tens of thousands. This is pretty much universally accepted by scientists, regulators, and reviewers.
What gets us out of this pandemic is nearly everyone getting some immunity, either naturally or through at least 1 shot. That's pretty much what happens with influenzas, and covid is probably headed in that direction. Some people will want or need an annual shot, just like the annual flu shot. Some people won't care for the shot. Some people in both groups will get sick, and some will die.
Upvote
14
(15
/
-1)
The biggest issue with this, is if the guy got admitted at the start of August (this being essentially the start of September) his infection is over, ivermectin isn't going to help. This is mostly dealing with the damage the infection did to his tissues.
I have no idea what I would do if presented with a court order to administer a drug that could potentially kill the patient (especially off-label). Well, I do know what I would do, which is stat-page our legal team! And I would equally want a court order that if this first order is executed that the court assumes all liability (informed that this will likely be lethal)
I have no idea what I would do if presented with a court order to administer a drug that could potentially kill the patient (especially off-label). Well, I do know what I would do, which is stat-page our legal team! And I would equally want a court order that if this first order is executed that the court assumes all liability (informed that this will likely be lethal)
Upvote
11
(11
/
0)
Statistical
Ars Legatus Legionis
Uh, "simple"? As a dual boarded physicia, trust me a multi-day written test is hardly simple... And all the people clamoring for his license getting revoked, don't seem to understand licensing and credentialing. That article doesn't mention if that doctor even has privileges at this ICU. I mean as a hospitalist my job is taking care of patients in the hospital for their outpatient providers. The outpatient providers (in general) have no ability to actually write an order that can be executed here in the hospital (I mean they can write a prescription all they want but that's an outpatient thing, I write orders - key difference is prescriptions are administered by the patient to themselves whereas orders are administered by the nurses to the patient). You need hospital privileges to do the latter but just a medical license and DEA # to do the former. But as an inpatient physician I am under no obligation to honor an outpatient prescription.Kind of irrelevant. The question is, as usual, why cannot we take away medical licenses when there is clear cause?That's ummm, disturbing.
And why is Dr. Wagshul still board certified?
Initial board certification is a simple test (also requires relevant residency experience). Mostly useful hanging on a wall, or seeking hospital privileges. Doesn't stop you from practicing medicine.
The article states the quack doctor does NOT have privilege at this or any other hospital.
But as an inpatient physician I am under no obligation to honor an outpatient prescription.
Which is what the entire article and case it about. The judge is trying to do just that FORCE the hospital in patient providers to implement the outpatient prescription.
Upvote
20
(20
/
0)
Not sure if I'm reading things wrong here (wouldn't be the first time, especially since English isn't my native tongue)Judges on the other hand, are expected to understand ethics.> "requested that the hospital doctors “administer Ivermectin pursuant to its dosage schedule,"
OK, the dosage schedule for COVID is 0 mg. Please administer 0 mg stat.
Then force this judge to retire.
the doctors need to rule the judge in contempt, and send him to prison.
Oh wait, they aren’t legal experts. Why should that stop them?
But I feel like ewelch was pointing out the wtf nature of this ruling since the judge (apparently) has even less idea about medicine than I do (and that's a low bar), overruling actual experts. Aren't doctors supposedly expected to understand ethics?
Like I said, I (probably) misunderstood something in this exchange =)
Upvote
0
(0
/
0)
blackhawk887
Ars Legatus Legionis
dude... please be smarter than this. This post alone makes me want to give up on the education system.
Covid is largely preventable. Even with the delta variant, we have 3 or 4 vaccines are effective enough that 100% vaccination (or even 90-95% vaccination coverage) would quickly and almost completely eradicate it.
Upvote
26
(26
/
0)
blackhawk887
Ars Legatus Legionis
People, even scientists, go absolutely nuts when talking about drugs. How is it ok to consume dangerous drugs like alcohol and tobacco, but forbidden to take ivermectin? There are absolutely no studies that prove ivermectin does or does not work. Why is it your decision, that of the fda or anyone else to dictate whether this drug can be given? Sorry folks, but the fda has gotten it wrong many many times. Need I cite the opioid epidemic and the massive over-prescribing of narcotics in very recent times? It should be my decision, and mine alone, to decide what drugs I take in extremis. Although I concede ivermection is unproven, does that mean I should be forbidden to take it if there is any chance whatsoever that it might help?
Hospitals and doctors have legal and ethical obligations to not harm patients. They are in no way obligated to give the patient any drugs they want.
Ivermectin is about 1,000 times as toxic as alcohol.
Next time I'm in the hospital, I wonder if they'll give me meth on demand?
It's worth a try. Maybe get a court order for it?
Upvote
11
(11
/
0)
If the news report I read is correct, the regimen indicated in the judge's order (30 mg/day for 3 weeks) is way off standard. 30 mg would be appropriate for a single dose for a 200 kg person. Typically the drug is only given as a single dose as an antiparasitic. There seems to be little chronic toxicity data. I found a Belgian case report of a woman with delusions of parasitic infection who took 12 mg of prescription tablets daily for two weeks. She was pretty generally ill and "she was confused and disoriented in time. On examination, she was effectively confused and apathic, with a slow and dysarthric speech. She presented myoclonia of the hands." Apparently she recovered after a few days. The case report didn't mention any lasting effects, but this whole thing is scary.
www[.]antigifcentrum[.]be/sites/default/files/imce/Poster_Ivermectin_vs03b_2014.pdf
www[.]antigifcentrum[.]be/sites/default/files/imce/Poster_Ivermectin_vs03b_2014.pdf
Upvote
18
(18
/
0)
Post content hidden for low score.
Show…
Holy jebus.. So far I'd only seen accounts of people of dying of covid just rejecting the whole thing, accusing doctors for being liars etc, this is the first time I've read about someone recognizing the fact and still, I guess, wanting to "own the libs"....and the Trumptardery continues on...
Now he is winner of a Darwin award."At first, Caleb refused to get tested for COVID-19, or go to the hospital.
"'He was so hard-headed,' Jessica [his wife] said. "'He didn't want to see a doctor, because he didn't want to be part of the statistics with COVID tests.'
"'Caleb instead began taking tablets of ivermectin (an anti-parasitic medicine the U.S. Food and Drug Administration has since urged people not to take for COVID-19), high doses of Vitamin C, zinc aspirin, and an inhaler. By July 30, however, Caleb was taken by a relative to the emergency room at Shannon Medical Center.'"
Edit. sad..

Upvote
8
(8
/
0)
Clearly a case of politically motivated overreach by the judge. It would be legitimate for a judge to order treatment if the medication or procedure was routine or established efficacious by clinical trials, but that is not the case here. The opposite, in fact: a trial was stopped because the treatment was statistically indistinguishable from a placebo. But in dystopian Amurica, it is now acceptable for politicians and judges to overrule doctors and scientists. And why not? For decades now, the fossil fuel industry has been overruling the scientific evidence for anthropogenic climate change. Why should a prerogative that is available to business be denied to politicians and judges?
Upvote
4
(4
/
0)
Statistical
Ars Legatus Legionis
Independent studies show promise for Ivermectin, if we look at actual data (a summarized site pooling all studies
If you summarize low quality studies you get low quality results.
If you summarize a mix of high and low quality studies, you also get low quality results.
The only way to get high quality meta-analyses is to restrict the review to high quality studies. We don't at the moment, have either of those.
And "shows promise" is a very low bar and not nearly enough to qualify as standard of care.
Not at all advocating for this being first course (or even advocating this at all for treatment) but not sure how we get past the politics of this and actually get what would be considered by, let's say you, high quality analysis.
I have no dog in the fight but I can say with 100% accuracy (anecdotally) which side of the political spectrum someone falls on based on this drug alone which doesn't make for good science. I don't think monthly booster shots get's us out of this pandemic so I welcome different ideas.
There is no politics in what constitutes a high quality medical study. It needs to be a clinical trial, it needs to be randomized and placebo controlled, it needs to examine relevant dosages, it needs to be double-blinded, and it needs a large sample size - at least thousands, preferably tens of thousands. This is pretty much universally accepted by scientists, regulators, and reviewers.
What gets us out of this pandemic is nearly everyone getting some immunity, either naturally or through at least 1 shot. That's pretty much what happens with influenzas, and covid is probably headed in that direction. Some people will want or need an annual shot, just like the annual flu shot. Some people won't care for the shot. Some people in both groups will get sick, and some will die.
I don't disagree with a lot of what you are saying but we went all out with the vaccine as if Covid-19 is like influenza A or B and it's not acting like the flu so we should be doing something different but we aren't... we are talking about boosters. I'm only suggesting we try something different and instead of shooting down treatments that, admittedly, have worked for a small sample size, we should do more testing. We literally have nothing to lose... people are dying regardless. I'm sure there are tens of thousands of infected that are anti-vaxxers that would be happy to sign up for such a trial (the patient in this article being one of them).
There already is a trial. It is unlikely to have more than a modest impact. Certainly not a substitute for vaccination. The patient is not indicated for the trial as his disease progression is too severe and his health too questionable. In fact being hospitalized completely excludes one from the trial entirely.
Once again we don't know if this drug will do anything to fight covid but IF it does it will be for early onset treatment. A drug to slow the spread of the virus enough to let the immune system catch up. Once the virus has fully propegated through the body the drug is unlikely to be useful. Any dosage high enough to disrupt the virus will be toxic to the host as well. Once again I caveat we don't even know for sure it does anything statistically significant that is the purpose of the trial and the vast majority of clinical trials fail.
Saying we have nothing to lose though isn't correct. Vaccination will save lives. Period. People clinging to false hope will get themselves killed. It may turn out that if ivermectin is useful it is useful in conjunction with vaccination. Of course it may be completely useless too and then the freedumbers will move on to the next hail mary "solution" when there is one cheap, easy, and scientifically proven - vaccination.
Upvote
20
(20
/
0)
blackhawk887
Ars Legatus Legionis
Independent studies show promise for Ivermectin, if we look at actual data (a summarized site pooling all studies
If you summarize low quality studies you get low quality results.
If you summarize a mix of high and low quality studies, you also get low quality results.
The only way to get high quality meta-analyses is to restrict the review to high quality studies. We don't at the moment, have either of those.
And "shows promise" is a very low bar and not nearly enough to qualify as standard of care.
Not at all advocating for this being first course (or even advocating this at all for treatment) but not sure how we get past the politics of this and actually get what would be considered by, let's say you, high quality analysis.
I have no dog in the fight but I can say with 100% accuracy (anecdotally) which side of the political spectrum someone falls on based on this drug alone which doesn't make for good science. I don't think monthly booster shots get's us out of this pandemic so I welcome different ideas.
There is no politics in what constitutes a high quality medical study. It needs to be a clinical trial, it needs to be randomized and placebo controlled, it needs to examine relevant dosages, it needs to be double-blinded, and it needs a large sample size - at least thousands, preferably tens of thousands. This is pretty much universally accepted by scientists, regulators, and reviewers.
What gets us out of this pandemic is nearly everyone getting some immunity, either naturally or through at least 1 shot. That's pretty much what happens with influenzas, and covid is probably headed in that direction. Some people will want or need an annual shot, just like the annual flu shot. Some people won't care for the shot. Some people in both groups will get sick, and some will die.
I don't disagree with a lot of what you are saying but we went all out with the vaccine as if Covid-19 is like influenza A or B and it's not acting like the flu so we should be doing something different but we aren't... we are talking about boosters. I'm only suggesting we try something different and instead of shooting down treatments that, admittedly, have worked for a small sample size, we should do more testing. We literally have nothing to lose... people are dying regardless. I'm sure there are tens of thousands of infected that are anti-vaxxers that would be happy to sign up for such a trial (the patient in this article being one of them).
There is an ongoing clinical trial studying this that is recruiting 15,000 people. I linked it upthread.
Covid is more deadly than the flu, but we have better vaccines for covid than we do for the flu... so the net out should be about the same level of spread and mortality, once everyone gets some immunity. Getting immunity via vaccine is VASTLY preferable to via infection.
Flus have be circulating for decades, so everyone has various levels of natural immunity to them, in addition to varying levels of vaccination. Usually this is enough to fight flus off, but in the old, young, and immune compromised it isn't always enough. Annual flu shots are essentially "boosters" (there's some terminology differences here, but for the purposes of this conversation they are close enough). Giving out covid boosters is treating it very much like we treat the flu.
Upvote
10
(10
/
0)
Independent studies show promise for Ivermectin, if we look at actual data (a summarized site pooling all studies
If you summarize low quality studies you get low quality results.
If you summarize a mix of high and low quality studies, you also get low quality results.
The only way to get high quality meta-analyses is to restrict the review to high quality studies. We don't at the moment, have either of those.
And "shows promise" is a very low bar and not nearly enough to qualify as standard of care.
Not at all advocating for this being first course (or even advocating this at all for treatment) but not sure how we get past the politics of this and actually get what would be considered by, let's say you, high quality analysis.
I have no dog in the fight but I can say with 100% accuracy (anecdotally) which side of the political spectrum someone falls on based on this drug alone which doesn't make for good science. I don't think monthly booster shots get's us out of this pandemic so I welcome different ideas.
There is no politics in what constitutes a high quality medical study. It needs to be a clinical trial, it needs to be randomized and placebo controlled, it needs to examine relevant dosages, it needs to be double-blinded, and it needs a large sample size - at least thousands, preferably tens of thousands. This is pretty much universally accepted by scientists, regulators, and reviewers.
What gets us out of this pandemic is nearly everyone getting some immunity, either naturally or through at least 1 shot. That's pretty much what happens with influenzas, and covid is probably headed in that direction. Some people will want or need an annual shot, just like the annual flu shot. Some people won't care for the shot. Some people in both groups will get sick, and some will die.
I don't disagree with a lot of what you are saying but we went all out with the vaccine as if Covid-19 is like influenza A or B and it's not acting like the flu so we should be doing something different but we aren't... we are talking about boosters. I'm only suggesting we try something different and instead of shooting down treatments that, admittedly, have worked for a small sample size, we should do more testing. We literally have nothing to lose... people are dying regardless. I'm sure there are tens of thousands of infected that are anti-vaxxers that would be happy to sign up for such a trial (the patient in this article being one of them).
We have a recipe that is guaranteed to work, even for Delta: vaccines + masks + moderate social distancing
Why should that be abandoned to try quack remedies? Now granted, there certainly are a ton of mouth breathers that seem to want to abandon a proven solution to try out nonsense, but popularity doesn't make a solution correct.
Saying that something 'worked' for small sample sizes is scientific nonsense. Something hasn't 'worked' until statistically you can trust the result.
Upvote
19
(19
/
0)
Why were you trying to remove her tubes etc?While obviously a tragedy for those involved, I find it all ironic.
So, thousands of patients in a study showing real efficacy of a vaccine, not good enough.
*no* supporting data, let me force you to give it to me.
The article didn't explicitly say he wasn't vaccinated, so it's possible it's a breakthrough case.
Could be, but it also sounds like it's not covid-19 that's causing most of his problems, but rather the infection he caused himself by trying to yank out his respirator and feeding tubes.
Which is another thing I don't understand. I've known people who've been intubated to that extent, and they were fully conscious and able to communicate via writing; it definitely wasn't pleasant for them, but none of them tried de-intubating themselves. There are lots of pieces missing from this story.
No. There's plenty of times someone in an ICU is conscious and able to communicate, but they're definitely not thinking clearly. I had to spend 4 days with my partner trying to remove her nasogastric tube, her neck cannula and then reiterating over and over that she wasn't in the ICU because someone had hurt her again. I was the one who had to give consent to medical procedures as there was no chance of her being in a state to assess anything.
Wasn't my most fun week to say the least.
I feel like I'm digging myself deeper with this one, but I'm hoping you (at least now that the situation isn't acute) can appreciate the ambiguous wording of your post with just a touch of humor.
I'm not known for my great sense of humor and I will accept all the downvotes
Upvote
-4
(2
/
-6)
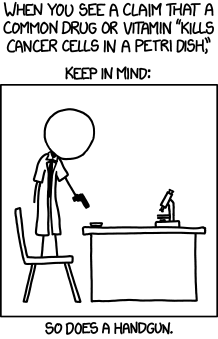
Relevant XKCD comic, just replace "cancer" with "SARS-CoV-2 virus":But people have clung to the idea that ivermectin can treat COVID after a study early in the pandemic suggested that it disrupted SARS-CoV-2’s ability to infect cells. What’s often overlooked is that study was limited to cells in Petri dishes.
Upvote
17
(18
/
-1)
this is one of the truly insidious parts of medical quackery, they can use misleading data from extremely small sample sizes even with legitimate studies, just by translating it to fractions or percentages, that's why there are collage level courses that are about understanding statistics, scientific papers on the higher level, and now they are putting emphasis on understanding them at a basic level for media courses, which are now lumped in with academics as part of the core classes, not necessarily prerequisites where im at, though it is for some, but a highly recommended optional for filling out credit hours to reach a full load.[
Note, also, that n=75 is divided into 3 separate arms: placebo, ivermectin plus doxycycline, and ivermectin alone. So the improvement claimed was only in 24 patients.
The authors themselves state no conclusions can be drawn from this study due to its extremely small size.
There's also the matter of the conflicting ivermectin plus doxycycline arm producing no results, a further indication that what's being measured is are noise fluctuations.
Studies with tiny sample sizes are a pet peeve of mine. I wish that studies with less than some significant sample size - maybe around a hundred, but more is always better - would either be rejected for peer review or accepted with the proviso that they carry a warning that their results are very likely meaningless. I see this a lot in dietary studies, too, and once a study involving 11 people with 6 of them showing some illusory improvement from Food X is published, it'll be flogged on Nutriblogs for eternity.
Yes, it's bad enough that the pharma industry makes decisions at the 2 sigma (95%) level; so bad, in fact, that the American Statistical Association issued a statement condemning it: https://amstat.tandfonline.com/doi/full ... t2XIOaE2MN. But the practice continues. The FDA and FTC, as appropriate, should take the position that any claims based on less than that level of confidence are prima facie evidence of fraud, and prosecute the offenders.
Upvote
0
(0
/
0)
blackhawk887
Ars Legatus Legionis
People, even scientists, go absolutely nuts when talking about drugs. How is it ok to consume dangerous drugs like alcohol and tobacco, but forbidden to take ivermectin? There are absolutely no studies that prove ivermectin does or does not work. Why is it your decision, that of the fda or anyone else to dictate whether this drug can be given? Sorry folks, but the fda has gotten it wrong many many times. Need I cite the opioid epidemic and the massive over-prescribing of narcotics in very recent times? It should be my decision, and mine alone, to decide what drugs I take in extremis. Although I concede ivermection is unproven, does that mean I should be forbidden to take it if there is any chance whatsoever that it might help?
There is no evidence ivermectin can help. Doctors aren't going to give you every random medicine you request just because you're desperate.
More to the point, this doctor is prescribing insane amounts of ivermectin, well beyond the accepted safe dosage.
I don't generally like the phrase "no evidence". Usually there is evidence, just no proof - to whatever standard of proof is required. Even when there is no direct evidence, there are usually relevant priors that we can and should consider when judging probabilities that something will or will not work.
Upvote
-8
(1
/
-9)
Iggy the Jiggy Piggy
Ars Tribunus Militum
There are legitimate uses for this drug. Is the off-label use affecting the supply of this drug? In the USA it's mostly used to treat parasites in animals. Summer is a peak time for said parasites.
Upvote
2
(2
/
0)
blackhawk887
Ars Legatus Legionis
Independent studies show promise for Ivermectin, if we look at actual data (a summarized site pooling all studies
If you summarize low quality studies you get low quality results.
If you summarize a mix of high and low quality studies, you also get low quality results.
The only way to get high quality meta-analyses is to restrict the review to high quality studies. We don't at the moment, have either of those.
And "shows promise" is a very low bar and not nearly enough to qualify as standard of care.
Not at all advocating for this being first course (or even advocating this at all for treatment) but not sure how we get past the politics of this and actually get what would be considered by, let's say you, high quality analysis.
I have no dog in the fight but I can say with 100% accuracy (anecdotally) which side of the political spectrum someone falls on based on this drug alone which doesn't make for good science. I don't think monthly booster shots get's us out of this pandemic so I welcome different ideas.
There is no politics in what constitutes a high quality medical study. It needs to be a clinical trial, it needs to be randomized and placebo controlled, it needs to examine relevant dosages, it needs to be double-blinded, and it needs a large sample size - at least thousands, preferably tens of thousands. This is pretty much universally accepted by scientists, regulators, and reviewers.
What gets us out of this pandemic is nearly everyone getting some immunity, either naturally or through at least 1 shot. That's pretty much what happens with influenzas, and covid is probably headed in that direction. Some people will want or need an annual shot, just like the annual flu shot. Some people won't care for the shot. Some people in both groups will get sick, and some will die.
I don't disagree with a lot of what you are saying but we went all out with the vaccine as if Covid-19 is like influenza A or B and it's not acting like the flu so we should be doing something different but we aren't... we are talking about boosters. I'm only suggesting we try something different and instead of shooting down treatments that, admittedly, have worked for a small sample size, we should do more testing. We literally have nothing to lose... people are dying regardless. I'm sure there are tens of thousands of infected that are anti-vaxxers that would be happy to sign up for such a trial (the patient in this article being one of them).
We have a recipe that is guaranteed to work, even for Delta: vaccines + masks + moderate social distancing
Why should that be abandoned to try quack remedies? Now granted, there certainly are a ton of mouth breathers that seem to want to abandon a proven solution to try out nonsense, but popularity doesn't make a solution correct.
Saying that something 'worked' for small sample sizes is scientific nonsense. Something hasn't 'worked' until statistically you can trust the result.
None of those things work as a treatment, though. These people desperately want an effective treatment, because either they already have covid, or they want to avoid vaccines, masking, distancing, or other prophylactic measures and an effective treatment would let them do that because people could just "get cured" even if they get sick.
Upvote
8
(8
/
0)
Brett's extracurriculars are not surprising... him, his brother, Jordan Peterson and the other "alt media" guys are arrogant, bellicose and on the edge of sanity.This is insane, and almost certainly an illegal and unenforceable order.
Re: Ivermectin, a study that shows high doses of the drug disrupt covid's ability to reproduce in a petri dish is interesting, and the kind of thing that should be followed up on... by a controlled study conducted by medical doctors and virologists, and reported on in a peer-reviewed journal. It should not be followed-up on by a bunch of people taking dangerous doses of the drug. It's insane.
I saw Brett Weinstein (who has been on the vanguard of "Ivermectin prevents covid!") speak once, a few years back, and he seemed to a be a reasonable, decent guy. He's obviously completely lost his mind over the course of the pandemic. It's depressing.
That said, I enjoyed that crowd a couple years ago. Interesting but weird people.
Upvote
4
(4
/
0)
Post content hidden for low score.
Show…
There's shortages in stores, an some farmers are unable to find a supply for their animals.There are legitimate uses for this drug. Is the off-label use affecting the supply of this drug? In the USA it's mostly used to treat parasites in animals. Summer is a peak time for said parasites.
https://www.abcactionnews.com/news/nati ... -treatment
One of the repercussions of the Ivermectin is that horse owners now have none to give their animals. Shelly Smith says she can't find a single supplier who has Ivermectin in stock right now, and she has no guarantee that will change anytime soon.
https://www.wtva.com/content/news/COVID ... 66781.html
Dr. Smith is also a beef cattle veterinarian working with the drug, Ivermectin, often.
He said without the use of the drug, the parasites could stunt animal growth and health.
“There is some concern that producers, people that are raising horses or cattle that the drug is intended for may not be able to have access to it when they need to,-” Smith stated.
Upvote
10
(10
/
0)
this is one of the truly insidious parts of medical quackery, they can use misleading data from extremely small sample sizes even with legitimate studies, just by translating it to fractions or percentages, that's why there are collage level courses that are about understanding statistics, scientific papers on the higher level, and now they are putting emphasis on understanding them at a basic level for media courses, which are now lumped in with academics as part of the core classes, not necessarily prerequisites where im at, though it is for some, but a highly recommended optional for filling out credit hours to reach a full load.[
Note, also, that n=75 is divided into 3 separate arms: placebo, ivermectin plus doxycycline, and ivermectin alone. So the improvement claimed was only in 24 patients.
The authors themselves state no conclusions can be drawn from this study due to its extremely small size.
There's also the matter of the conflicting ivermectin plus doxycycline arm producing no results, a further indication that what's being measured is are noise fluctuations.
Studies with tiny sample sizes are a pet peeve of mine. I wish that studies with less than some significant sample size - maybe around a hundred, but more is always better - would either be rejected for peer review or accepted with the proviso that they carry a warning that their results are very likely meaningless. I see this a lot in dietary studies, too, and once a study involving 11 people with 6 of them showing some illusory improvement from Food X is published, it'll be flogged on Nutriblogs for eternity.
Yes, it's bad enough that the pharma industry makes decisions at the 2 sigma (95%) level; so bad, in fact, that the American Statistical Association issued a statement condemning it: https://amstat.tandfonline.com/doi/full ... t2XIOaE2MN. But the practice continues. The FDA and FTC, as appropriate, should take the position that any claims based on less than that level of confidence are prima facie evidence of fraud, and prosecute the offenders.
Is it weird that the pharma industry is OK with 2-sigma tolerances while our manufacturing industries are still embracing 6-sigma?
Upvote
4
(4
/
0)
Maybe he's a readerWho do you think we are? John Oliver?This is the FLCCC's propaganda site. https://covid19criticalcare.com/
I am not saying that people with a certain set of skills arsians are likely to have should do anything to it. But I wouldn't be upset if they did.
Upvote
1
(1
/
0)
blackhawk887
Ars Legatus Legionis
but to say "vaccination will save lives", while maybe true for the flu I don't even think that's provable for Covid-19 yet as we see vaccinated individuals contracting it and dying (for one instance see the Massachusetts outbreak where 75% of those infected were vaccinated".) And I'm not suggesting at all that vaccines for Covid shouldn't be taken I'm stating that it's not enough.
It is 100% absolutely provable that the covid vaccines are saving lives. Every vaccine has breakthrough infections, and some of those will result in deaths, but definitely, absolutely, far fewer deaths than there would be in a 100% unvaccinated population. Anyone claiming otherwise is making several math or stats errors, because this isn't even close to a serious or supportable contention.
The flu vaccines also have a lot of breakthroughs and deaths. Other vaccines have far fewer, but still some. The difference is mainly the number of variants and the number of infections. Measles, for example, is very rare, so it causes very few deaths. Flu is very common and has more variants, so it sneaks around vaccines and causes far more deaths.
Upvote
17
(17
/
0)
As a nurse I've had to explain to residents that just because something is written as an order, doesn't mean I have to do it. If I think something is going to hurt my patient, my legal duty per my liscenceure is to not do it. If they want it done they either have to convince me it's safe or come down and do it themselves. ( Usually they are ordering something at 3am that would make sense for a lot of people, just not for people with leukemia with no WBC or PLT, like IM meds) I said to one "you can write an order for me to stab a guy, but I'm not going to stab a guy". I highly doubt that what ever court this ends up in is going to say the opinion of one rando judge trumps the legal requirements of a medical license. I'm going to assume that the judge in question has never even looked at the liscenceure language or scope of practice of any medical personnel. I mean that judge actually thinks that this one fiat can undo the whole set of regulations governing medical personnel. Does he have any clue as to how many people had to agree to those standards, debate them, ratify them? And we talk about surgeons having a God complex. Ppft. I hope someone puts him in his place soon.
Upvote
20
(20
/
0)
Fancy Internet Person
Ars Tribunus Angusticlavius
Uh, "simple"? As a dual boarded physicia, trust me a multi-day written test is hardly simple... And all the people clamoring for his license getting revoked, don't seem to understand licensing and credentialing. That article doesn't mention if that doctor even has privileges at this ICU. I mean as a hospitalist my job is taking care of patients in the hospital for their outpatient providers. The outpatient providers (in general) have no ability to actually write an order that can be executed here in the hospital (I mean they can write a prescription all they want but that's an outpatient thing, I write orders - key difference is prescriptions are administered by the patient to themselves whereas orders are administered by the nurses to the patient). You need hospital privileges to do the latter but just a medical license and DEA # to do the former. But as an inpatient physician I am under no obligation to honor an outpatient prescription.Kind of irrelevant. The question is, as usual, why cannot we take away medical licenses when there is clear cause?That's ummm, disturbing.
And why is Dr. Wagshul still board certified?
Initial board certification is a simple test (also requires relevant residency experience). Mostly useful hanging on a wall, or seeking hospital privileges. Doesn't stop you from practicing medicine.
The prescribing doctor does not have any privileges at the hospital.
He has never seen the patient.
His business is that for $90 (I think), he will talk to you on the phone and then prescribe HCQ or Ivermectin (whichever you pick on their website).
https://americasfrontlinedoctors.org/tr ... edication/
Upvote
26
(26
/
0)
- Status
- Not open for further replies.